-Benign Prostatic Hyperplasia (BPH)-

-Benign Prostatic Hypertrophy (BPH) presents with polyuria, nocturia, hesitancy, urgency and weak urinary stream.
-Symptoms of BPH appear gradually over a number of years
-Incidence increase with age
-BPH is not believed to be a risk factor for prostate cancer
-Differential diagnosis includes: urethral stricture, bladder neck contracture, carcinoma of the prostate, carcinoma of the bladder, bladder calculi, urinary tract infection, prostatitis, and neurogenic bladder
-Recommended test is urinalysis and serum PSA and renal panel
-patients with symptoms should have a digital rectal exam to assess prostate size and detect nodules and malignancy
-Optional tests include maximal urinary flow rate (normal > 15 mL/sec), post residual urine volume, and urine cytology
-Many agents used for treatment of BPH
-Alpha 1 Adrenergic Antagonists (Terazosin, Doxazosin, and Tamsulosin) act against the dynamic component of bladder outlet obstruction by relaxing smooth muscle in the bladder neck, prostate capsule, and the prostatic urethra
-5 Alpha Reductase Inhibitors (Finasteride and Dutasteride) act by reducing the size of the prostate gland
-Patients with frequency, urgency, and incontinence may be due to an overactive bladder
-Surgical treatment for BPH includes TURP (transurethral resection of the prostate)
-Open Prostatectomy can be for those who fail TURP
-Urethral stent may be effective for selected patients
-Congenital Abnormalities-
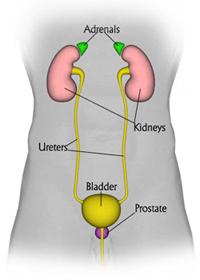
-Renal Agenesis- is almost always unilateral and does not cause symptoms. It is when the kidney is absent or underdeveloped
-Renal Hypoplasia-this appears as one small kidney with the other one larger than normal. Small kidneys have small arteries that can lead to hypertension. A nephrectomy maybe needed to correct this.
-Supernumerary Kidneys-third kidney is very rare and not be confused with the relatively common unilateral duplication of the renal pelvis
-Renal Dysplasia and Multicystic Kidney-multicysic kidney is usually only seen in one kidneys and is an irregularly lobulated mass of cysts and usually absent or atretic ureter. Usually associated with other abnormalities such as a ureteropelvic junction obstruction. Dysplasia of the renal parenchyma is seen with urethral obstruction or reflux present in early pregnancy or obstructed ureter
-Simple Renal Cyst-can be inherited or acquired. Significant renal damage is rare but usually requires only continuous followup.
-Renal Fusion-the most frequent abnormality seen is a horseshoe kidney containing two excretory system and two ureters
-Ectopic Kidney-with a simple ectopic kidney the kidney does not ascend properly and is found in the pelvis or over the brim. It is prone to infection and obstruction. Less common is crossed ectopy without fusion.
-Ureteral Atresia-the ureter may be absent or fail to extend to the bladder. It is associated with ipsilateral absent or multicystic kidney. Bilateral atresia is incompatible with life
-Duplication of ureter-one of the most common congenital malformations. It is often asymptomatic but may have recurrent UTI's
-Ureterocele-this is a sacculation of the bladder end of the ureter that can occur either in the bladder or ectopically. It may be asymptomatic or causes obstruction, incontinence or infection.
-Ectopic Urethral Orifice-usually occurs with ureterocele and duplication of the ureter but single ectopic ureters are seen. Males may get epididymitis because ureter drains into the vas deferens
-Obstructed Mega Ureter-caused by obstruction at the UVJ
-Bladder Exstrophy-the absence of the anterior wall of the bladder, with the ureters delivering urine into the lower abdomen. Requires surgical correction
-Persistent urachus-this appears as a draining umbilical sinus and can become infected
-Contraction of the Bladder Neck-common cause of reflux, bladder diverticulae or irritable bladder
-Apenia -absence of a penis. Rare.
-Megalopenis- the penis enlarges rapidly in childhood due to high levels of production of testosterone
-Micropenis-small but otherwise normally formed penis with a stretched length of less than 2.5 standard deviation below the mean.
-Urethral Stricture-severe case can result in damage to the bladder and hydronephrosis due to back pressure of the urine
-Hypospadias-urethral meatus found on the underside of the penis.
-Epispadias- this is a defect of the dorsal wall of the urethra. The urethra is displaced dorsally so that it opens on the top of the penis in males
-Labial Fusion-fused labia minora causing recurrent infections as a result of obstruction to urinary flow
-Clitoral Hypertrophy-this is caused by exposure to fetal androgens
-Polycystic Kidney Disease-the most common cause of serious renal inherited disease. It is an autosomal dominant condition.
-Medullary Sponge Kidney-can affect one or both kidneys. There are ectatic and cystic changes of the medullary and papillary collecting ducts.
-Potter's Syndrome-describes the typical physical appearance caused by pressure in utero due to oligohydraminos due to bilateral renal agenesis
-Cryptorchidism-
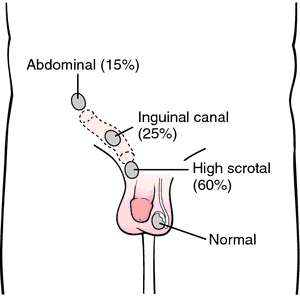
-Most cyrptorchid testes are undescended but some are absent due to agenesis or atrophy
-True undescended testes have stopped short along their normal path of descent into the scrotum
-Cryptorchism is defined as testis not in the scrotum not descended into the scrotum by four months of age
-In most instances referral is appropriate if testicles not descended between 6-12 months of age
-Complications of undescended testicles include inguinal hernia, testicular torsion, testicular trauma, subfertility, and testicular cancer.
-Surgery is recommended ASAP after the child is 6 months of age and should definitely be completed before 2 years of age
-Orchioplexy is the procedure of choice for repositioning palpable undescended testicles
-Exploratory surgery is recommended for non palpable undescended testis
-Erectile Dysfunction-

-Erectile Dysfunction (ED) is defined as the consistent or recurrent inability to acquire or sustain an erection of sufficient rigidity and duration for sexual intercourse
-Risk factors for ED include: obesity, smoking, watching television, dyslipidemia, obstructive sleep apnea, prescription meds (SSRI's spironolactone, clonidine, methyldopa, thiazide diuretics, cimetidine, and ketoconazole) and cardiovascular disease
-Other factors may lead to ED such as psychosocial factors (depression and stress), neurological (spinal cord injuries, MS, or dementia), bicycling, testosterone deficiency, hyperthyroidism, hyperprolactinemia, and hypothyroidism
-Normal erections require blood flow from the hypogastric arterial system into erectile chambers. High levels of intrapenile nitric oxide act as a local neurotransmitter to facilitate the relaxation and cause erection
-Treatment includes Phosphodiesterase-5 Inhibitors (PDE-5)-including sildenafil, vardenafil, and tadalafil
-These all act to increase intracavernosal cyclic GMP levels, and each one has been proven to be effective in restoring erectile dysfunction.
-There is intrapenile injection options with PDE-5 inhibitors as well as vacuum devices available if these other methods are not an option.
-Hydrocele/Varicocele-

-Hydrocele is a collection of peritoneal fluid between the parietal and visceral layers of the tunica vaginalis, the investing layer that directly surrounds the testis and the spermatic cord
-Hydroceles are believe to arise from an imbalance of the secretion and reabsorption of fluid form the tunica vaginalis
-Symptom of hydrocele of pain and disability and increasing size of the mass
-Hydroceles can be from epididymitis, torsion, appendiceal torsion, and can be idiopathic
-Ultrasound can be used when the diagnosis is in question
-Surgical excision is the most common treatment of hydrocele
-Varicocele is caused by a dilation of the pampinform plexus of the spermatic veins.
-Varicocele occurs in the left hemiscrotum usually
-Symptoms of varicocele include dull, aching left scrotal pain, typically worse when standing better when setting
-Varicocele can cause decreased fertility
-Treatment of varicocele surgical treatment ligating the gonadal vein so that retrograde blood flow can no longer reach the plexus of veins in the scrotum.
-Urinary Incontinence-

-Urinary incontinence is the involuntary leaking of urine
-4 main types of urinary incontinence are urge, stress, mixed, and overflow incontinence
-The types of incontinence overlap
-Cause of urinary incontinence: UTI, those that originate from the urinary tract, those caused by a systemic condition (diabetes mellitus), and those from a reversible cause (medications)
-Urgency incontinence have symptoms of incontinence accompanied by urgency. Partly caused by detrusor overactivity
-Stress incontinence have involuntary leakage that occurs with effort, sneezing, coughing laughing, and anytime there is an increase in intra-abdominal pressure
-Overflow incontinence is involuntary, continuous leakage or dribbling and incomplete bladder emptying. Caused by impaired detrusor contractility or bladder outlet obstruction
-Look for potentially reversible causes
-Need bladder stress test, post void residual volume and urodynamic testing
-Surgery may be helpful for stress incontinence and other instances
-Weight loss can decrease the episodes of stress incontinence
-Bladder retraining can help with urgency, stress, or mixed incontinence
-Kegel exercises are effective for urgency, stress, and mixed incontinence
-Continence pessaries may be used for stress incontinence
-Antimuscarinics such as darfenacin, fesoterodine, oxybutin, solifenacin, and tolterodine are effective for urgency and mixed incontinence or overactive bladder
-Other modalities include electrical stimulation and magnets
-Surgery is a last resort for intractable urgency incontinence
-Nephrolithiasis/Urolithiasis-
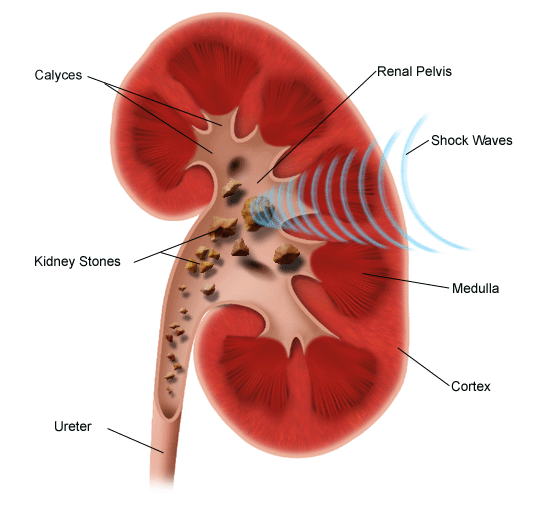
-Several types of kidney stones: calcium oxalate, calcium phosphate, uric acid, cysteine and struvite stones
-Calcium Oxalate stones are the most common kidney stones. Risk factors for development include low urine volume, higher urine calcium excretion, higher urine oxalate excretion, and lower urine citrate excretion
-Calcium phosphate stones make up about 15 percent of stones and can be seen in combination with calcium oxalate or struvite stones. Risk factors include lower urine volume, higher urine calcium excretion, lower urine citrate excretion, higher urinary pH, and higher urine phosphate excretion.
-Uric acid stones are radiolucent. Risk factors include lower urine volume, high urine uric acid excretion, and lower urine pH
-Struvite stones only form in the presence of urease producing bacteria (proteus). High urine pH and infection are risk factors for development of these struvite stones.
-Presenting symptoms typically include flank pain radiating to lower abdomen, nausea, vomiting, dysuria, hematuria, and polyuria. May have fever and chills accompanying it.
-90 percent of stones less than 4 mm will pass with a couple weeks.
-Kidney stones greater than 5 mm is associated with decrease in spontaneous passage rate
-Initial workup should include CBC, BMP, and Urinalysis. Imaging studies CT scan without contrast is ideal, but if radiation exposure is a concern renal ultrasound can demonstrate hydronephrosis and shadows which can indicate the presence of stones.
-Analgesics Toradol is ideal if not pregnant, bleeding is not a concern, and renal function is intact. Morphine and Dilaudid can be used as adjuncts. Zofran or Phenergan for nausea.
-Flomax 0.4 mg daily has been shown to relax ureter and help with spontaneous passage of stone
-If stones are septic and obstructing emergent decompression of the collecting system is needed with percutaneous drainage or ureteral stenting with antibiotics (cipro or rocephin)
-Surgical therapy for stones that do not or cannot pass spontaneously include lithotripsy, stenting, or basket retrieval
-Paraphimosis/Phimosis-
-Paraphimosis-refers to retracted foreskin in an uncircumcised or partially circumcised glans penis that cannot be returned to its normal position
-Phimosis-a tight foreskin that cannot be retracted to expose the glans penis. Can be normal or physiologic in young children. Older adults may get infections such as balanoposithis or inflammatory scarring
-Paraphimosis can cause impairment of venous and lymphatic flow from the constricting ring and cause engorgement of the glans penis and swelling. The arterial flow becomes compromised over hours to days. Penile necrosis, infarction of the glans, or gangrene can occur
-Treatment consists of timely reduction of the foreskin over the glans penis and requires pain control
-Testicular Torsion-

-Testicular torsion is a urologic emergency that is most common in neonates and post pubertal boys
-Testicular torsion can occur at any age
-Testicular torsion results from the inadequate fixation of the testis to the tunica vaginalis. The testis may twist on the spermatic cord causing ischemia from reduced arterial blood flow and venous obstruction
-Testicular torsion may be from trauma or can occur spontaneously. Can also reduce spontaneously and be occur intermittently
-It is generally felt that testis suffered irreversible damage after twelve hours of torsion.
-Clinically there is usually sudden onset of pain occurs usually after several hours of vigorous activity or minor trauma. There can be nausea and vomiting.
-Classic exam finding include a asymmetric high riding testis on the affected side with the long axis of the testis oriented transversely instead of longitudinally secondary to shortening of the spermatic cord. This is called a Bell Clapper deformity
-Diagnosis is made by ultrasound
-Treatment is surgery and involves detorsion and fixation
-If surgery is over two hours from happening attempts at manual detorsion should be attempted by rotating outward toward the thigh.
No comments:
Post a Comment